

SUBSCRIBE TO OUR FREE NEWSLETTER
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
5
#000000
#FFFFFF
To donate by check, phone, or other method, see our More Ways to Give page.
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.

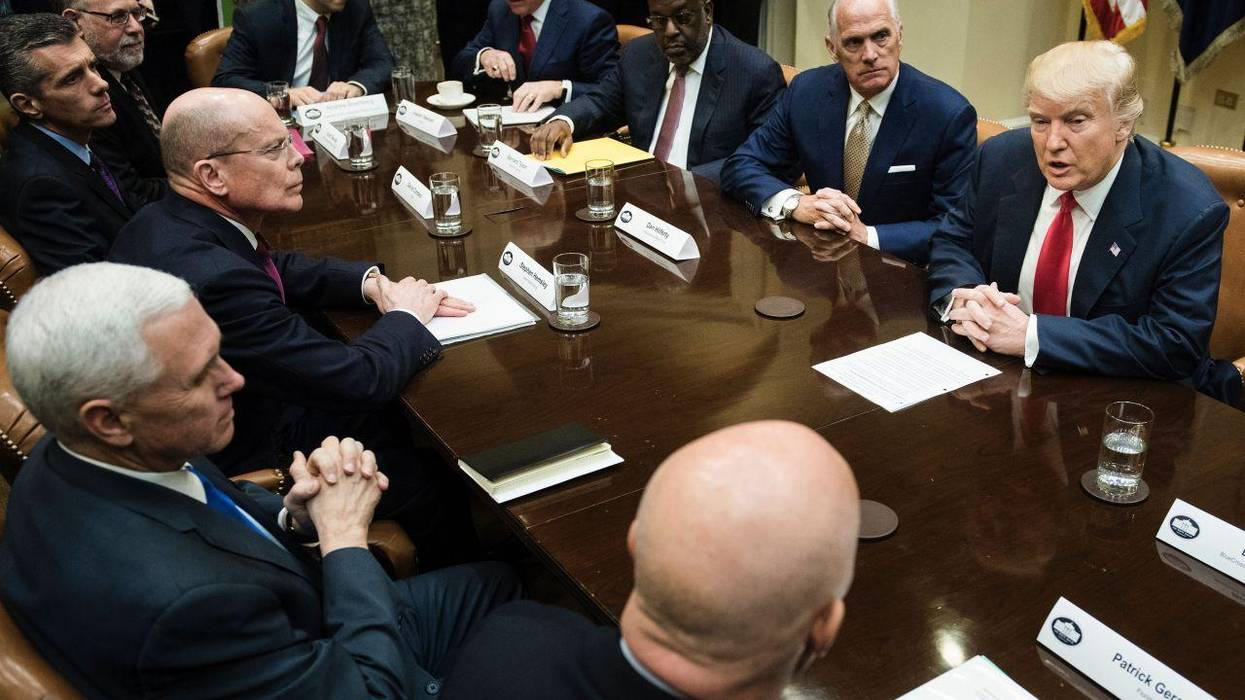
Don Dempsey would join Centers for Medicare and Medicaid Services nominee Mehmet Oz and other supporters of privatized Medicare Advantage plans in the new administration.
U.S. President Donald Trump is reportedly set to appoint a lobbyist for the for-profit health insurance industry for a top White House budget job, a move likely to heighten concerns about the new administration's expected push to bolster Medicare Advantage plans that deny necessary care and dramatically overbill the federal government.
The Financial Times reported Wednesday that Trump is "poised to appoint" Don Dempsey as associate director of the Office of Management and Budget's health programs. The appointment would give Dempsey "sweeping power over the $1.8 trillion U.S. healthcare budget and responsibilities of the 13 divisions and agencies," the newspaper noted.
Dempsey is currently the vice president of policy and research at the Better Medicare Alliance, a lobbying organization that describes itself as "the nation's leading research and advocacy organization supporting Medicare Advantage." FT observed that the group is "funded by insurance companies including UnitedHealth Group and Humana"—the two largest Medicare Advantage insurers in the United States.
Trump's reported choice represents another potential boon for Medicare Advantage, a program run by private insurers and funded by the federal government. As STAT reported last month, "Medicare Advantage insurers thrived under the first Trump administration, and it's expected to happen again now that Trump is returning to the White House and Republicans are taking control of Congress."
The president has nominated Mehmet Oz, who has previously expressed support for a plan dubbed "Medicare Advantage for All," to lead the Centers for Medicare and Medicaid Services (CMS), a move that one watchdog warned would kick Medicare privatization efforts "into overdrive."
Since his inauguration earlier this week, Trump has taken a number of steps that have alarmed healthcare advocates, including rescinding Biden-era executive orders aimed at lowering prescription drug prices and strengthening Medicaid and the Affordable Care Act.
"On one hand, what we see coming from the executive orders by Trump is important because it shows us the direction they are going with policy changes," Sarah Lueck, vice president for health policy at the Center on Budget and Policy Priorities, told KFF Health News. "But the other track is that on the Hill, there are active conversations about what goes into budget legislation. They are considering some pretty huge cuts to Medicaid."

The U.S. "has always accepted that we are the country that overpays relative to the rest of the world," said one health policy expert.
The Biden administration's Medicare drug price negotiations yielded lowered costs for 10 commonly used drugs, and the White House said last month that Americans would save an estimated $1.5 billion in out-of-pocket expenses thanks to the talks—but an analysis out Tuesday found that the U.S. will still be paying far more than other wealthy countries.
Reuters reviewed the maximum prices that Australia, Japan, Canada, and Sweden have agreed to pay for nine of the 10 drugs for which Medicare negotiated prices this year, and found that the U.S. will still be paying more than double the amount for the medications on average.
The new prices are set to go into effect on January 1, 2026, but two of the highest prices the U.S. will still pay are for Imbruvica, for blood cancers, and Stelara, for conditions including Crohn's disease and psoriasis.
Medicare will be charged $9,319 for a 30-day supply of the latter drug, compared to $4,607 in Sweden. For Stelara, the U.S. will pay $4,695 under the negotiated prices—more than four times the amount it costs in Sweden, Australia, and Canada.
For Enbrel, which treats conditions including arthritis, Medicare will pay $2,355 per month—far less than the list price of $7,106, but still more than $1,000 over what Sweden is charged: $709. Australia pays $573, while Canada pays $704, and Japan pays just over $300 for the drug.
"The government negotiations are especially significant for drugs where market forces were most limited and therefore had the least impact on producing price concessions."
Stacie Dusetzina, a professor of health policy at Vanderbilt University, told Reuters that the U.S. has "always accepted that we are the country that overpays relative to the rest of the world."
The analysis comes two weeks after the Brookings Institution published a review of the impact of the United States' first federal negotiations of prescription drug prices, finding that just three of the drugs which had little competition in the market accounted for more than half of the $6 billion the U.S. is expected to save in 2026.
"The government negotiations are especially significant for drugs where market forces were most limited and therefore had the least impact on producing price concessions," said Brookings.
Reuters noted that in other countries, prices generally come down over time, but U.S. drugmakers are able to raise prices annually and often extend patents by making small changes to medications, stopping less expensive generic versions from hitting the market and saving patients money.
Unlike in other wealthy countries, Johns Hopkins Bloomberg School of Public Health scientist Mariana Socal told Reuters, "the longer a drug is in the U.S. market, the more we pay."
With previous list prices well into the hundreds and thousands for the 10 drugs included in negotiations so far, Medicare agreed to pay close to $200 for a 30-day supply for drugs including Xarelto, Jardiance, and Farxiga—medications for which other governments examined by Reuters pay $78 or less, thanks to their longstanding negotiations.
The RAND Corporation found in a study in February that before the Medicare negotiations were included in the Inflation Reduction Act, U.S. health plans paid more than three times as much as other countries for brand-name drugs, even after discounts.
"A contributor to higher U.S. per capita drug spending is faster uptake of new and more expensive prescription drugs in the United States relative to other countries," wrote researchers at the London School of Economics in a study in 2013. "In contrast, the other OECD countries employed mechanisms such as health technology assessment and restrictions on patients' eligibility for new prescription drugs, and they required strict evidence of the value of new drugs."
The researchers suggested pharmaceutical companies in the U.S., like in other countries, should be required "to provide more evidence about the value of new drugs in relation to the cost" and negotiate prices accordingly.
As Merith Basey, executive director of Patients for Affordable Drugs, said in August after the results of the first round of negotiations were announced, advocates are still pushing for far more savings in upcoming talks between Medicare and drug manufacturers, which are expected to start next year.
"We remain committed to expanding the Medicare negotiation program to more drugs," said Basey last month, "and fighting for additional reforms to lower drug prices for all patients who need relief."

"Health insurance coverage has expanded in America, but we are finding it is private health insurance corporations themselves that are often the largest barrier for people," said one organizer.
A day after 150 people assembled outside the headquarters of UnitedHealth Group to demand the for-profit health insurance giant stop its "systemic" denial of coverage, the company announced Tuesday the huge profits it raked in over the second quarter of 2024: $7.9 billion.
The sum, said one organizer, exemplifies why the demonstrators were willing to risk arrest to speak out against the firm's practices.
"UnitedHealth Group's $7.9 billion quarterly profit announcement is the result of a business model built on pocketing premiums and billions of dollars in public funds, then profiting by refusing to authorize or pay for care," said Aija Nemer-Aanerud, Health Care for All campaign director for People's Action Institute. "People should not have to turn to public petitions or direct actions to get UnitedHealthcare to pay for the care they need to live. That makes no sense, unless you're a shareholder or executive eyeing your next big luxury purchase."
Eleven people were detained by police at Monday's demonstration, where they blocked the street in front of UnitedHealth's headquarters in Minnetonka, Minnesota, displaying signs that read, "United (Denies) Healthcare" and "The Price Is Wrong."
The demonstration was organized by the Care Over Cost campaign at People's Action Institute, which has worked to help people across the country overturn care denials by UnitedHealth and other for-profit insurance giants.
Gina Morin of Auburn, Maine spoke at the event about having her mental health treatment denied by her Medicare Advantage plan administered by UnitedHealth.
"Two years ago my therapist was denied payment for seven of my mental health sessions she provided," she said. "I tried to pay her even though I'm on a limited income and she wouldn't take the money. If my provider, in her professional opinion, believed I needed those therapy sessions, who is UnitedHealth to deny coverage?"
As Common Dreams reported last month, UnitedHealth was named in a letter written by 52 members of the Democratic caucus in Congress as one of the healthcare companies that use artificial intelligence to decide via algorithm that coverage should be provided or denied to patients who have Medicare Advantage plans, which are billed as offering coverage that traditional Medicare doesn't include.
ProPublica reported last year on Christopher Naughton, a man with ulcerative colitis whose treatment cost $2 million per year, leading UnitedHealth to flag his account as "high dollar." The company contracted with a doctor to review Naughton's case, and the doctor found the treatment for symptoms including arthritis, debilitating diarrhea, and blood clots was "not medically necessary."
After suing the company, Naughton's family found UnitedHealth had lied about what Naughton's personal physician told the contractor in order to come to their conclusion and end coverage.
"Health insurance coverage has expanded in America, but we are finding it is private health insurance corporations themselves that are often the largest barrier for people to receive the care they and their doctor agree they need," Nemer-Aanerud told CBS News Monday.
In April, People's Action sent a letter to UnitedHealth noting that its CEO was paid nearly $10 million in 2022 while the CEO of its parent company "extracted over $90 million in executive and board pay for himself" over four years.
The company took $22.4 billion in profits in 2023 and sent $14.8 billion to shareholders through stock buybacks and dividends—yet continues to deny necessary healthcare coverage to its members.
The group called on UnitedHealth to:
"Citizens mobilized against corporate abuses in the 1960s and 70s. It can happen again now."
Most heads of giant corporations are drunk with their own power. These corporate CEOs push the envelope in ways that harm defenseless people. They believe they can get away with anything, and they do, with few exceptions. The few corporate crime prosecutions keep declining from Obama to Trump to Biden, due to a settlement-obsessed Department of Justice staffed by lawyers readying to join the lucrative major corporate crime defense firms.
Corporate law firms, which deserve far more scrutiny by the media, have over the decades built a wall of immunity and impunity around these giant firms and their self-enriching CEOs. These CEOs now make an average of $14,000 an hour, while employing workers who are lucky to make $20 an hour. Greedy CEOs have surpassed the lords of medieval feudalism in the disparity they impose on workers.
Corporate law firms find Congressional lawmakers receptive to their campaign contributions and services in drafting legislative loopholes. These law firms place business executives and their own law partners in high executive branch positions (See, Servants of the Damned: Giant Law Firms, Donald Trump, and the Corruption of Justice by David Enrich, 2022).
Corporate law firms specialize in creating an edifice of secretive, anonymous corporate registries that attract a majority of big U.S. corporations to charter in Delaware. Companies register hundreds of shell companies (LLCs) for evasive purposes. Delaware law firms write the corporate law of Delaware for the rubber stamp state legislature. Ironically, these corporate capitalists disempower their own shareholders. Wall Street firms, credit card companies and tax escapees love Delaware. (See, What’s the Matter with Delaware?: How the First State Has Favored the Rich, Powerful, and Criminal – and How It Costs Us All by Hal Weitzman, 2022).
New outrages that swell the corporate crime wave are disclosed daily. Most exposés go nowhere, due to a lazy Congress (about ready again to take off most of the summer until after Labor Day) and to patsy regulators and meager, inadequate enforcement budgets funded by the corporate Congress.
One regular, no longer so patsy, is the tiny Federal Trade Commission (FTC) with an annual budget of $430 million. FTC Chair Lina Khan has just sued giant Amazon (annual sales of $524.89 billion) in the words of New York Times reporter, David McCabe “for illegally inducing consumers to sign up for its Prime services and then hindering them from canceling the subscription…”
The FTC charged that “Amazon tricked and trapped people into recurring subscriptions without their consent’ ‘… duped millions of consumers … [and with] manipulative, coercive or deceptive’ design tactics on its website.” Amazon’s lawyers, of course, deny everything.
On other matters, corporate lawyers are going berserk flexing their obstructive muscles. They sued the state of California for passing a law mildly protecting children from social media-produced harm. Susan Linn in her new book, “Who’s Raising the Kids? Big Tech, Big Business, and the Lives of Children” documents the abuses perpetrated by high predators.
Not to be outdone by their peers, corporate lawyers for the drug industry just filed a frivolous lawsuit against the U.S. Government that was finally authorized by Congress to allow ripped-off Medicare officials to negotiate drug prices with the overcharging Big Pharma. (The VA and the Pentagon already have the power to negotiate with the drug companies.) Presumably, having U.S. taxpayers continue to pay by far the highest drug prices in the world through Medicare—charged by subsidy-coddled U.S. drug companies—suits the “pay or die” Big Pharma CEOs.
Moreover, U.S. drug companies are happy to offshore to China the production of antibiotics. Our country produces virtually no antibiotics – a national security peril I wrote about to President Biden and Secretary of Defense Lloyd Austin, that received no response to date. (See: Letter to President Joe Biden – June 2, 2023).
ProPublica has exposed the giant Cigna health insurance company for rejecting millions of patients’ claims through its hired doctors who instantly deny coverage “on medical grounds” without opening the patient file.” (See, https://www.propublica.org/article/cigna-pxdx-medical-health-insurance-rejection-claims). This report, based on corporate documents and interviews with former Cigna physicians, has not led to any prosecutions either by state or federal officials. This is an egregious example of CEOs pushing the envelope and getting away with it.
A New York Times investigation by Sarah Kliff et al. revealed that a wealthy nonprofit hospital network – Allina Health – in the Midwest has been denying regular health care for patients who have unpaid medical bills. They have cut off patients, “including children and those with chronic illnesses like diabetics and depression.” Canadians, with their universal Medicare system, are stunned when they learn that many hospitals in the U.S. aggressively sue indebted patients, garnish their wages and seize their tax refunds. This is worse than debtors’ prisons where those incarcerated might receive health care.
Anyone who thinks corporate crimes are committed by just a few bad apples in the barrel can read my book Getting Steamed to Overcome Corporatism: Build It Together to Win (2011). Getting Steamed is an enraging compilation of documented corporate crime and criminogenic behavior – resulting in the loss of life, injuries and money from consumers and workers. One of the best public corporate crime databases is Violation Tracker, a project of Good Jobs First. Violation Tracker has over half a million entries that include civil and criminal actions against corporate wrongdoing. (See, https://violationtracker.goodjobsfirst.org/). In addition, visit the Corporate Crime Reporter website https://www.corporatecrimereporter.com/ to see highlights of crime in the suites each week.
Earlier this month, the Justice Department, which after decades of declining to have a comprehensive public corporate crime database, finally launched a modest database. (See: https://www.justice.gov/corporate-crime/corporate-crime-case-database).
Why don’t the American people rise up and tell their legislators and law enforcers that they will no longer accept the terrible corporate harm inflicted on them daily? This harm includes dangerous products (Opioids), detrimental services (medical negligence leading to 5000 deaths per week, according to a John Hopkins School of Medicine peer-reviewed report), toxic pollution, workplace casualties, endless cheating of consumers ($350 billion in health industry billing fraud a year) and other intolerable abuses. (See Malcolm Sparrow’s website: https://scholar.harvard.edu/msparrow).
Most corporate crooks are above the law. They think that collectively “We the People” are a nation of sheep – unable and unwilling to take their demands, often supported by large majorities, to Congress and get some strong law and order legislation enacted. Polls show huge majorities (left/right) want jail time and restitution from wealthy corporate outlaws.
Public Citizen, which lobbies against corporate crime, wants to hear from you (visit, https://www.citizen.org/). PC’s president Robert Weissman, together with former PC president Joan Claybrook, have a new book coming out next month. It’s called “The Corporate Sabotage of America’s Future: And What We Can Do About It.” Read it and generate a rumble all the way to your congressional senators and representatives who are about to head home as Congress goes into recess for most of the summer.
Citizens mobilized against corporate abuses in the 1960s and 70s. It can happen again now when the corporate overlords in the context of demonstrated crises – climate, pandemics and powerful unregulated technologies – are acting far worse than they have in recent times.
The awakened power of dedicated, informed people cannot be overcome.

"We must act to end the international embarrassment of the United States being the only major country on earth to not guarantee healthcare to all," said Sen. Bernie Sanders.
Economic justice and human rights advocates applauded Wednesday as progressives in the U.S. House and Senate reintroduced legislation to expand the Medicare system to all Americans, with the bill garnering more support in Congress than ever before.
More than half of the Democratic caucus in the House has signed on as co-sponsors of the Medicare for All Act of 2023, including 13 powerful ranking members of congressional committees.
Sen. Bernie Sanders (I-Vt.) was joined by Reps. Pramila Jayapal (D-Wash.) and Debbie Dingell (D-Mich.) in leading more than 120 lawmakers in introducing the bill, with a number of supporters speaking about the worsening healthcare crisis at a press conference on Capitol Hill.
"We live in a country where millions of people ration lifesaving medication or skip necessary trips to the doctor because of cost," said Jayapal. "Sadly, the number of people struggling to afford care continues to skyrocket as millions of people lose their current health insurance as pandemic-era programs end. Breaking a bone or getting sick shouldn't be a reason that people in the richest country in the world go broke."
"There is a solution to this health crisis—a popular one that guarantees healthcare to every person as a human right and finally puts people over profits and care over corporations," the congresswoman added. "That solution is Medicare for All—everyone in, nobody out."
About 15 million people in the U.S. are set to lose their health coverage this year as pandemic-era assistance ends, adding to the 85 million people who are currently either uninsured or underinsured—with coverage that includes high deductibles and other out-of-pocket costs, leaving them unable to afford the healthcare they need.
Sanders, who has advocated for a government-run health program for decades, noted in a press statement than 68,000 people per year in the U.S. die due to a lack of health coverage.
"The American people understand, as I do, that healthcare is a human right, not a privilege," said Sanders, who serves as chairman of the Senate Health, Education, Labor, and Pensions Committee. "As we speak, there are millions of people who would like to go to a doctor but cannot afford to do so. That is an outrage... We must act to end the international embarrassment of the United States being the only major country on earth to not guarantee healthcare to all."
Under the Medicare for All Act, the existing Medicare program—which is generally open only to people age 65 and older—would be expanded to everyone in the United States and would allow them to obtain primary, vision, dental, reproductive, and mental healthcare; prescription drugs; substance abuse treatment; long-term healthcare services; and other medical care without any cost at the point of service.
While detractors—including lawmakers who take substantial donations from the for-profit health insurance industry—have frequently claimed that Medicare for All would be too expensive, a Congressional Budget Office analysis found in 2020 that the program would save between $300 billion and $650 billion annually.
"A study by RAND found that moving to a Medicare for All system would save a family with an income of less than $185,000 about $3,000 a year, on average," said Sanders' office in a statement.
The lawmakers introduced the legislation a day after Sanders and Jayapal hosted a town hall on Capitol Hill where they were joined by patients, doctors, and nurses whose experiences in the U.S. healthcare system illustrate the need for Medicare for All.
Dr. Natasha Driver, a first-year obstetrics and gynecology resident at Howard University Hospital in Washington, D.C., said she recently cared for a woman whose service industry job did not provide her with health insurance.
"When I first met her after delivery, she refused treatments which were part of routine postpartum care for the simple reason that she couldn't afford them," said Driver. "This is a regrettable and all too common occurrence in the practice of medicine, especially for those of us who work with the underserved. Medicare for All would reduce the problem of uninsurance and allow me to adequately care for my patients."
Robert Weissman, president of consumer advocacy group Public Citizen, noted that while millions of Americans lack health coverage that would allow them to receive adequate care, health insurers, hospital chains, and pharmaceutical companies "are generating staggering profits," with insurance companies making more than $69 billion last year.
"It's time for Americans to stop being treated like suckers. It's time to make healthcare a right. It's time for Medicare for All," said Weissman. "A system of expanded and improved Medicare for All would reduce our spending on healthcare while providing universal access, better outcomes, and more equity."
"With Medicare for All, healthcare decisions would be made by patients and doctors—not for-profit insurance companies thinking about their bottom lines," he added. "There would never be another medical bankruptcy. Having decent coverage would not depend on where a person works or whether they are employed or married. Patients could take their prescriptions on schedule, without worrying about price."
Social Security Works (SSW) pointed out that the legislation is being introduced as Republicans threaten the Medicare and Social Security systems with their proposal to raise the debt ceiling in exchange for social spending cuts.
"Medicare for All's supporters envision a future where Medicare is improved to include dental, hearing, vision and long-term care, and then expanded to cover everyone in America," said Alex Lawson, executive director of SSW. "A future without delays or denials, without copays or deductibles. A future where everyone gets the care they need. Meanwhile, Republicans want to make our current profit-driven healthcare system even worse."
"The best way for Democrats to stop that from happening," Lawson said, "is to go on offense with full-fledged support for Medicare for All."

The number of uninsured Americans has dropped to an all-time low. But that fact obscures the failures of our patchwork, profit-driven healthcare system.
Here's one of many indicators about how broken the United States healthcare system is: Guns seem to be easier and cheaper to access than treatment for the wounds they cause. A survivor of the recent mass shooting in Half Moon Bay, California, reportedly said to Gov. Gavin Newsom that he needed to keep his hospital stay as short as possible in order to avoid a massive medical bill. Meanwhile, the suspected perpetrator seemed to have had few obstacles in his quest to legally obtain a semi-automatic weapon to commit deadly violence.
Americans are at the whim of a bewildering patchwork of employer-based private insurance plans, individual health plans via a government-run online marketplace, or government-run healthcare (for those lucky enough to be eligible). The coverage and costs of plans vary dramatically so that even if one has health insurance there is rarely a guarantee that there will be no out-of-pocket costs associated with accessing care.
It's hardly surprising then that the latest Gallup poll about healthcare affirms what earlier polls have said: A majority of Americans want their government to ensure health coverage for all. In fact, nearly three-quarters of all Democrats want a government-run healthcare system.
Gallup also found that a record high number of people put off addressing health concerns because of the cost of care. Thirty-eight percent of Americans said they delayed getting treatment in 2022—that's 12 percentage points higher than the year before. Unsurprisingly, lower-income Americans were disproportionately affected.
Women are especially impacted, with more women than men delaying treatment as per the same Gallup poll. The findings were consistent with results published by researchers at New York University's School of Global Public Health, which found that women's healthcare was increasingly unaffordable, compared to men's—in a study that solely focused on people with employer-based health coverage. Imagine how out-of-reach healthcare is for uninsured women.
Added to that, Republican-led abortion bans have made it even harder for American women to obtain reproductive healthcare. On the 50th anniversary of the recently overturned Supreme Court decision Roe v. Wade, abortion providers in Massachusetts, for example, reported a steady stream of people driving to their state—one where abortion remains legal—to access care.
President Joe Biden and the Democratic Party appear to think that this grim status quo is perfectly acceptable. Democrats' reliance on the Obama-era Affordable Care Act (ACA) as a bulwark against Republican opposition to any government intervention in healthcare seems to be resoundingly successful—at least on paper. In December 2022, Biden touted the fact that 11.5 million Americans, a record high number, had signed up for ACA plans during the last enrollment period. He said, "Gains like these helped us drive down the uninsured rate to eight percent earlier this year, its lowest level in history."
His administration, rather than working to fulfill what a majority of his party's constituents want—a government-run healthcare system—has continued instead to tweak the ACA by extending a period of discounted monthly premiums for private insurance plans. Such tweaks are not permanent. Neither are they a panacea for accessing adequate care. If anything, they are a façade protecting profit-based private insurance companies.
A survey by the Commonwealth Fund found that although the number of insured Americans is now at an all-time high, more than 40% of those who bought ACA plans and nearly 30% of those with employer-based plans were underinsured—that is, the plans were inadequate to cover their healthcare needs.
By focusing solely on the number of people who had health plans as a measure of success, the White House is participating in a great coverup of the ongoing American healthcare tragedy.
Meanwhile, just over the horizon from Biden's celebration of record numbers of ACA signups is the fact that millions of people currently enrolled in the Medicaid government health plan could lose access because of the end of an emergency provision that allowed for "continuous enrollment." That provision expires at the end of March 2023. If all Americans were automatically enrolled in government-provided healthcare regardless of eligibility, this would not be a concern.
Right-wing sources, so terrified that too many Americans want a government-run health system, are busy shaping public opinion against it. The Pacific Research Institute's Sally Pipes recently published an op-ed about how Canada's national health system was a good reason why the United States should not have a similar program. Using the deadly logic of a free marketeer, she wrote, "In Canada, healthcare is 'free' at the point of service. As a result, demand for care is sky-high."
The implication is that charging people for service would reduce the demand, just as it would for, say, an electric vehicle. In Pipes' world, people are accessing healthcare just for fun, and if they were charged money for it, their ailments might resolve themselves without treatment.
The Heritage Foundation also published an attack on Britain's National Health Service (NHS), gleefully claiming that it is "cratering," and warning that it is a lesson for American liberals who might support a similar "single-payer" system in the United States.
The Wall Street Journal's editorial board published a similar warning, claiming that the NHS was "failing patients, with deadly consequences."
It's puzzling why the Pacific Research Institute, Heritage Foundation and Wall Street Journal appear unconcerned about the 330,000 Americans who lost their lives during the Covid-19 pandemic simply because they don't live in a nation with a universal healthcare program.
The United States spends nearly twice as much per capita on healthcare than other comparable high-income nations. According to Health Affairs, excessive administrative costs are the main reason for this discrepancy—these are non-medical costs associated with delivering healthcare in a patchwork system of employer-based private health and publicly subsidized plans. In fact, "administrative spending accounts for 15 – 30 percent of health care spending."
Again, right-wing media outlets and think tanks appear unconcerned by this disturbing fact. They only want to convince Americans that a government-run health plan is a bad idea. And, sadly, the Democratic Party leaders like Biden seem to agree.
The National Union of Healthcare Workers, together with Healthy California Now, created an online calculator for individuals to determine how much money they would save if the United States had a single-payer system.
I have an employer-based healthcare plan that is considered very good. Using the calculator, I determined that I would save more than $16,000 if California, the state where I live, had a single-payer system. That's money I could be saving for my children's higher education or for my retirement.
The victims of mass shootings, like the Half Moon Bay survivor, are saddled with high costs of care on top of the trauma of having been shot. Every year, there are more than 80,000 survivors of injuries from firearms in the United States. Having a single-payer healthcare system would not fix our epidemic of gun violence. But it would certainly make it easier to bear.
Canada and Britain's state-run systems of health care may be imperfect, but they are a vast improvement on the survival-of-the-fittest approach that the United States takes.
Nonpartisan, publicly funded media is "an idea that we should explore," said the senator.
Appearing on "Face the Nation" on CBS Sunday, U.S. Sen. Bernie Sanders discussed a number of issues he covers in his upcoming book, It's OK to Be Angry About Capitalism, including his proposal to ensure the news media acts in the interest of the general public and not wealthy corporations and powerful interest groups.
Host Margaret Brennan described his proposal as "a New Deal for journalism."
As some European countries do, the Vermont Independent senator said, the U.S. should have "nonpartisan public funding of media" to ensure local news outlets can stay afloat and keep communities informed about "their city council, their school board."
Such a system would also prevent news networks like CBS from relying on advertising dollars, which Medicare for All advocates have blamed for playing a role in the corporate media's hostility towards a nationalized healthcare system and other progressive proposals for the public good.
"What I say in the book is that look, I've done 1,000 interviews, like I'm doing with you right now," Sanders told Brennan. "And nobody has ever come up to me, not one reporter—not you, not anybody else—and said, 'Bernie, why are we spending twice as much on healthcare as any other country and yet we have 85 million uninsured or underinsured?' How many programs at CBS, NBC, ABC had on why we have a dysfunctional healthcare system? Does that have anything to do with who owns the major networks? 'Bernie, what are you going to do about income and wealth inequality?' ... 'Why are billionaires paying an effective tax rate lower than working class people?' No one asked me those questions."
As Luke Savage reported at Jacobin following the 2020 presidential election, viewers of the Democratic primary debates weren't informed by moderators that Medicare for All was supported by a majority of Americans, and ad breaks featured "health insurance and pharmaceutical companies seizing every opportunity to bombard viewers with misleading industry agitprop about the breathtaking wonders of profit-driven healthcare."
He added:
CNN’s Detroit debate is a case in point; the network was demanding at least $300,000 from companies advertising, with a single thirty-second spot costing an estimated $110,000—and groups like the so-called Partnership for America’s Health Care Future (in practice, a front for various corporate interests), filled out many of the slots. Regardless of how anchors or hosts think about an issue like healthcare, the networks' basic model essentially precludes meaningful critique of the status quo by design. As long as it persists, don't expect to see the public interest or popular opinion reflected anywhere on cable TV.
To counter that dynamic, Sanders argued on "Face the Nation," a New Deal for journalism including publicly funded media is "an idea that we should explore."
In the interview, the senator spoke about his support for attaching "some strings" to U.S. funding for Israel to help pressure the country to end its human rights abuses against Palestinians.
Sanders also reiterated his call for the Democratic Party to focus on representing the interests of all working people.
"What we need to do is have a movement of Black workers, Latino workers, white workers, gay workers, straight workers, and understand that we're all in this together," said Sanders. "I don't care if you're living in rural Iowa, where I spent a lot of time, alright, you can't afford health care, you can't afford to send your kid to college, or you're living in San Francisco. So too often we forget about the economic issues that unite us. The vast majority of the people know the pharmaceutical industry is ripping us off. The vast majority of the people understand that we have to improve our educational system. Let's work on that."

A victim of the mass shooting in Half Moon Bay, California told Gov. Gavin Newsom that he wanted to leave the hospital as quickly as possible to avoid high medical costs.
An anecdote told by California Gov. Gavin Newsom at a press conference on the mass shooting in Half Moon Bay—the second such appearance he made in two days, following another deadly shooting in Monterey Park—encapsulated the United States' twin crises of economic injustice and rampant gun violence, said advocates on Monday.
The Democratic governor told the press that while visiting a man who'd been injured in the shooting at two farms in the Bay Area city, the victim said he was hoping to leave the hospital quickly to avoid high medical bills.
"He said, 'Hey, Governor, thanks for being here but when am I gonna get the hell out of here?'" Newsom said. "His leg was shattered by the gunfire. He goes, 'I can't afford to spend any more time here, I don't have the money."
"How many people are shot and then face massive medical debt? How much revenue and profit do hospitals generate via shootings? Perversity through and through."
The man's mother and son later arrived and told Newsom they were "worried he's going to lose his job at a warehouse the next day unless he can go back to work."
Politico reporter Lara Korte relayed the governor's comments on social media, eliciting numerous responses in which critics—including advocates for Medicare for All and strict gun control—said the post represented "the United States of America in one tweet."
"This is the most American tweet of all time," added progressive commentator Kyle Kulinski.
The shooting in Half Moon Bay was one of dozens of shootings since 2023 began just over three weeks ago. Along with the shooting in Monterey Park last Saturday and the shooting of a family in Enoch, Utah on January 4, it was one of the deadliest attacks so far.
Dr. Adam Gaffney, an intensive care unit doctor and former president of Physicians for a National Health Program, called Newsom's story "a gut-wrenching indictment of our healthcare system."
Dania Palanker, an assistant research professor at the Center on Health Insurance Reforms at Georgetown University's McCourt School of Public Policy, noted that the costs associated with being one of the millions of Americans who will survive gun violence in their lifetime are an often-overlooked consequence of the Republican Party's obstruction as the vast majority of Americans call for stricter gun control.
As CNN reported in December, one insured survivor of the mass shooting at Club Q in Colorado Springs received a bill for $130,000, while another person who was among the 27.5 million Americans who lack health insurance was billed $20,000 for spending a night in the emergency room where doctors stitched a bullet wound in his leg.
The Journal of the American Medical Association published a study last May showing that the average initial hospital charge for mass shooting survivors between 2012 and 2019 was nearly $65,000 per person.
"How many people are shot and then face massive medical debt?" asked physician and anthropologist Eric Reinhart. "How much revenue and profit do hospitals generate via shootings? Perversity through and through."

"Banks have identified medical credit cards as a lucrative opportunity to profit off of the worsening crisis of patients who are unable to afford their medical care," warned Sens. Elizabeth Warren, Ed Markey, Bernie Sanders, and others.
A group of progressive senators raised alarm this week over a pernicious outgrowth of the United States' for-profit healthcare system: medical credit cards.
In a letter to the chief executives of Wells Fargo and Synchrony Financial—two large issuers of medical credit cards—Sens. Elizabeth Warren (D-Mass.), Ed Markey (D-Mass.), Bernie Sanders (I-Vt.), Chris Murphy (D-Conn.), and Sherrod Brown (D-Ohio) expressed concern that "given the circumstances in which these cards are used, medical credit cards could be predatory to patients seeking medical care and leave patients stuck paying higher costs with 'hefty, high-interest debt.'"
"The concern here is the current structure of our healthcare system often requires that patients enter into medical debt in order to access services they need," reads the letter, which was made public this week. "Within that context, patients—often under duress because of concerns about their medical care—are being pushed into and then locked into medical credit cards despite the availability of alternative payment options that might be more beneficial and offer lower interest rates."
By contrast, medical credit cards often come with high interest rates following so-called "no interest" periods that banks deceptively use to lure in customers who are desperate to pay for costly medical treatments. In 2013, the Consumer Financial Protection Bureau (CFPB) ordered CareCredit—Synchrony Financial's medical credit business—to refund up to $34.1 million to "consumers who were victims of deceptive credit card enrollment tactics."
Last month, the CFPB hit Wells Fargo—which offers a medical credit card named Health Advantage—with $3.7 billion in penalties for a slew of abuses and called the institution "one of the most problematic repeat offenders of the banks and credit unions."
Crain's Chicago Business recently reported that "as healthcare costs and insurance deductibles rise, more hospitals in Chicago and around the country are teaming up with banks to market medical credit cards and other loans to patients who lack the insurance or funds to pay for care."
"Hospitals that convince patients to take medical credit cards get paid upfront by banks at a time when unpaid bills are straining their budgets. Lenders, for their part, see an opportunity to capitalize on the growing gap between the cost of medical care and what many Americans can afford," the newspaper continued. "Patients who take the card get money to pay for care, solving a short-term dilemma. But a quick decision made in a high-stress situation can create long-term financial problems. Patients who can't drum up the cash to pay off the initial balance within an introductory period end up with hefty credit card debt that carries some of the highest interest rates in the industry."
More than 100 million people are saddled with medical debt in the United States, collectively owing upwards of $200 billion.
Last year, Kaiser Health News spotlighted the story of Cheyenne Dantona, whose situation is appalling but increasingly common in the United States, where obtaining lifesaving treatment often entails financial ruin:
Dantona, 31, was diagnosed with blood cancer while in college. The cancer went into remission, but when Dantona changed health plans, she was hit with thousands of dollars of medical bills because one of her primary providers was out of network.
She enrolled in a medical credit card, only to get stuck paying even more in interest. Other bills went to collections, dragging down her credit score. Dantona still dreams of working with injured and orphaned wild animals, but she's been forced to move back in with her mother outside Minneapolis.
"She's been trapped," said Dantona's sister, Desiree. "Her life is on pause."
"The cards may also adversely impact consumers' credit reports because of the way they are treated by credit reporting agencies: the agencies recently agreed to remove 70% of medical debt from credit reports, but these changes will not benefit medical credit card holders because their debt is considered credit card debt and as such is 'viewed less favorably by the bureaus,'" the lawmakers wrote.
"Banks have identified medical credit cards as a lucrative opportunity to profit off of the worsening crisis of patients who are unable to afford their medical care," the lawmakers continued, demanding that the bank executives provide information about their medical credit card businesses such as how many accounts are in collections and how many healthcare providers they have partnered with.
"As we work to reform our healthcare system so no individual faces medical debt," the senators added, "we remain concerned about circumstances that serve only to exacerbate financial harm of unaffordable healthcare."
Sanders, a letter signatory and the incoming chair of the Senate Health, Education, Labor, and Pensions Committee, has decried the "very concept" of medical debt, arguing it "should not exist."
During his 2020 presidential campaign, Sanders offered a proposal to wipe out existing medical debt in the United States.
"In the wealthiest country in the history of the world," the senator said at the time, "one illness or disease should not ruin a family's financial life and future."