

SUBSCRIBE TO OUR FREE NEWSLETTER
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
5
#000000
#FFFFFF
To donate by check, phone, or other method, see our More Ways to Give page.
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
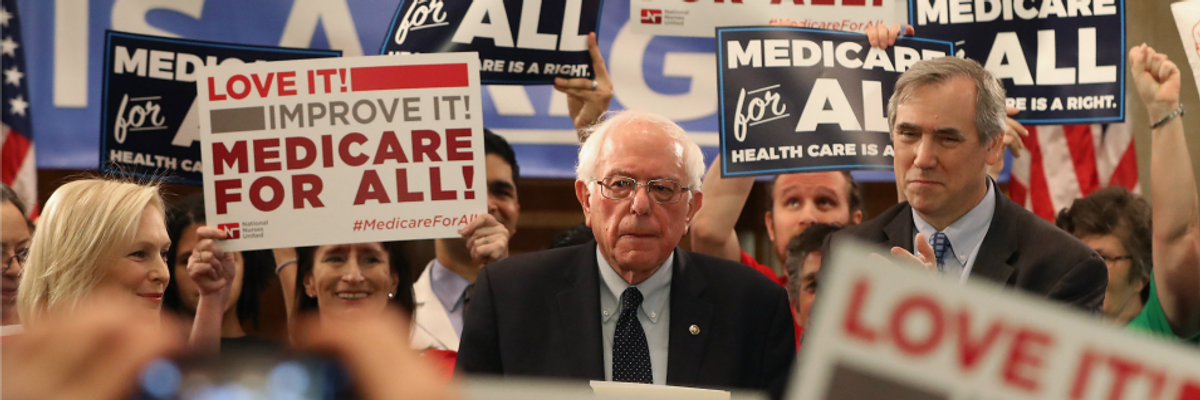
Sen. Bernie Sanders (I-Vt.) speaks while introducing healthcare legislation titled the "Medicare for All Act of 2019" with Sens. Kirsten Gillibrand (D-N.Y.) and Jeff Merkley (D-Ore.) during a news conference on Capitol Hill, on April 9, 2019 in Washington, D.C. (Photo: Mark Wilson/Getty Images)
The Congressional Budget Office issued a report on May 1, 2019 titled "Key Design Components and Considerations for Establishing a Single-Payer Health Care System." This report reviews a range of considerations as regards the design and implementation of a single- payer system as applied to the United States. The Medicare for All bills currently before both the U.S. House of Representatives and Senate, as introduced by Representative Pramila Jayapal and Senator Bernie Sanders respectively, both advocate the adoption of a single-payer system for the U.S.
The CBO report (pdf) properly examines both the positive potential as well as matters of concern in establishing a single-payer system in the U.S. As the report states, "A single-payer system would present both opportunities and risks for the health care system."
Overall, the CBO report, as with all such analyses, needs to address two fundamental issues with respect to the establishment of a single-payer system for the U.S. These are: 1) Is a single-payer system capable of providing good-quality care to all U.S. residents; and 2) Is a single-payer system capable of significantly reducing overall U.S. health care costs while still delivering universal good-quality care? The report does not provide explicit answers, yes or no, to these questions. But it does present a framework for understanding how the U.S. could, in fact, establish a successful single-payer system.
"A single-payer system would provide coverage for the 114 million U.S. residents who are presently either uninsured or underinsured. Healthcare outcomes for these 114 million people--35 percent of the U.S. population--will therefore almost certainly improve under a single-payer system."
It is crucial to provide some context for recognizing the potential of a U.S. single- payer system as presented within the CBO report. It is especially illuminating to consider some basic indicators on the operations of the current U.S. health care system in comparison with those of other high-income economies. Thus, as of 2017, the U.S. spent $3.3 trillion on health care. This equaled 17 percent of US GDP, with average spending at about $10,000 per person. By contrast, Germany, France, Japan, Canada, the UK, Australia, Spain and Italy spent between 9 - 11 percent of GDP on health care, averaging between $3,400 - $5,700 per person. Yet, by most measures--including those based on the "amenable mortality rate," which tracks medically preventable deaths--average health outcomes in all of these countries are superior to those in the UnitedStates.
The most basic cause of this poor U.S. performance is inadequate access to good- quality care. Roughly 9 percent of the U.S. population, 28 million people, are uninsured. Another 26 percent, 86 million people, are underinsured--i.e. they have insurance but are unable to access medical care because their deductibles or co-pays are prohibitively high. A large share of the remaining 65 percent of the population who are adequately insured still face high costs as well as anxiety over whether they could manage financially when they face any serious health issue.
Within this context, how, then, does the CBO assess the prospects for a U.S. single-payer system delivering good-quality universal coverage as well as significantly reduced overall health-care spending? We can summarize their perspectives briefly.
Good-quality universal coverage
The CBO is clear, first of all, that a single-payer system would achieve universal coverage, in dramatic contrast with our present system. The report states, "People who are currently uninsured would receive coverage and some people who are currently insured could receive additional benefits under the single-payer system, depending on its design." In other words, a single-payer system would provide coverage for the 114 million U.S. residents who are presently either uninsured or underinsured. Healthcare outcomes for these 114 million people--35 percent of the U.S. population--will therefore almost certainly improve under a single-payer system.
The CBO does not take an explicit position as to whether a single-payer system will also deliver benefits for the 65 percent of the population which presently has full health-insurance coverage. On the one hand, the report does note both the prospects for both improved outcomes as well as reduced costs as regards this population cohort, observing that:
Unlike private insurers, which can experience substantial enrollee turnover over time, a single-payer system without that turnover would have a greater incentive to invest in measures to improve people's health and in preventive measures that have been shown to reduce costs.
It is also the case that both the Jayapal and Sanders bills offer more extensive coverage than is currently provided under a typical employer-sponsored policy, including significant support for long-term care. Expanding coverage in such ways should further improve overall health outcomes for those already insured. But the CBO also recognizes that the expansion of coverage to the uninsured and underinsured will entail increased overall demands on the country's supply of health care resources. It is therefore possible, as the report notes, that this could produce shortages in terms of availability of providers, which, in turn, could mean reductions in quality of care. This is a legitimate issue which the CBO has properly highlighted.
More specifically, the single-payer system will need to be capable of establishing measures through which the provision of provider services can increase to match the increased demand resulting from universal coverage. I examined this question in depth in a 200-page peer-reviewed study with co-authors released last November, "Economic Analysis of Medicare for All." In our study, we conclude that a single-payer system will produce major reductions in the administrative burdens throughout the whole health-care system. The CBO report also recognizes this prospect for major reductions in administrative burdens under single-payer. These dramatic cuts in administration will then mean significantly less paperwork for doctors and nurses, freeing them to spend more time treating patients. On balance, our study concluded that this effective increase in the providers' available time to treat patients should roughly match the increased demand for their services resulting from universal coverage.
Reducing Health-Care Costs
Much of the CBO report is focused around specific issues in designing the payment system. These include: provider payment methods; global budgets; capitated payments; payment rates for providers; and the setting of prescription drug prices. These are all critical concerns, and the CBO report is now a valuable resource in summarizing them. But the report does not take a position as to whether a U.S. single-payer system will be able to successfully control costs. Rather, the study concludes that:
The cost of a single-payer system would depend on various design choices such as the services covered, cost-sharing requirements, and provider payment rates.
In addition to those design choices, policymakers could consider using two other techniques to contain the growth of government spending on the single-payer plan and total health care spending: global budgets and utilization management. (p.26)
The CBO assessment here is indisputable. It is therefore incumbent on the designers of a single-payer system to consider the range of design choices with great care, to achieve the potential cost savings that are available through a well-designed system. It is evident from comparing the U.S. health care system with those of other high-income economies that there is massive potential for cost savings in the U.S. system, with, as noted above, the comparison countries spending between 9 - 11 percent of GDP on health care while the U.S. spends 17 percent. Within the present U.S. economy, every percentage point of GDP amounts to roughly $200 billion. Thus, even reducing our current health care spending by 2 percentage points relative to GDP would yield an astronomical $400 billion in savings, even while our healthcare system budget, as a share of GDP, would remain far above those of other advanced economics.
The CBO study is therefore to be commended for describing a range of measures through which a U.S. single-payer system can successfully implement significant cost savings while still delivering good-quality care for all residents. As such, the CBO study makes a positive contribution toward understanding the possibilities for creating a fair and workable health care system in the United States.
Trump and Musk are on an unconstitutional rampage, aiming for virtually every corner of the federal government. These two right-wing billionaires are targeting nurses, scientists, teachers, daycare providers, judges, veterans, air traffic controllers, and nuclear safety inspectors. No one is safe. The food stamps program, Social Security, Medicare, and Medicaid are next. It’s an unprecedented disaster and a five-alarm fire, but there will be a reckoning. The people did not vote for this. The American people do not want this dystopian hellscape that hides behind claims of “efficiency.” Still, in reality, it is all a giveaway to corporate interests and the libertarian dreams of far-right oligarchs like Musk. Common Dreams is playing a vital role by reporting day and night on this orgy of corruption and greed, as well as what everyday people can do to organize and fight back. As a people-powered nonprofit news outlet, we cover issues the corporate media never will, but we can only continue with our readers’ support. |
The Congressional Budget Office issued a report on May 1, 2019 titled "Key Design Components and Considerations for Establishing a Single-Payer Health Care System." This report reviews a range of considerations as regards the design and implementation of a single- payer system as applied to the United States. The Medicare for All bills currently before both the U.S. House of Representatives and Senate, as introduced by Representative Pramila Jayapal and Senator Bernie Sanders respectively, both advocate the adoption of a single-payer system for the U.S.
The CBO report (pdf) properly examines both the positive potential as well as matters of concern in establishing a single-payer system in the U.S. As the report states, "A single-payer system would present both opportunities and risks for the health care system."
Overall, the CBO report, as with all such analyses, needs to address two fundamental issues with respect to the establishment of a single-payer system for the U.S. These are: 1) Is a single-payer system capable of providing good-quality care to all U.S. residents; and 2) Is a single-payer system capable of significantly reducing overall U.S. health care costs while still delivering universal good-quality care? The report does not provide explicit answers, yes or no, to these questions. But it does present a framework for understanding how the U.S. could, in fact, establish a successful single-payer system.
"A single-payer system would provide coverage for the 114 million U.S. residents who are presently either uninsured or underinsured. Healthcare outcomes for these 114 million people--35 percent of the U.S. population--will therefore almost certainly improve under a single-payer system."
It is crucial to provide some context for recognizing the potential of a U.S. single- payer system as presented within the CBO report. It is especially illuminating to consider some basic indicators on the operations of the current U.S. health care system in comparison with those of other high-income economies. Thus, as of 2017, the U.S. spent $3.3 trillion on health care. This equaled 17 percent of US GDP, with average spending at about $10,000 per person. By contrast, Germany, France, Japan, Canada, the UK, Australia, Spain and Italy spent between 9 - 11 percent of GDP on health care, averaging between $3,400 - $5,700 per person. Yet, by most measures--including those based on the "amenable mortality rate," which tracks medically preventable deaths--average health outcomes in all of these countries are superior to those in the UnitedStates.
The most basic cause of this poor U.S. performance is inadequate access to good- quality care. Roughly 9 percent of the U.S. population, 28 million people, are uninsured. Another 26 percent, 86 million people, are underinsured--i.e. they have insurance but are unable to access medical care because their deductibles or co-pays are prohibitively high. A large share of the remaining 65 percent of the population who are adequately insured still face high costs as well as anxiety over whether they could manage financially when they face any serious health issue.
Within this context, how, then, does the CBO assess the prospects for a U.S. single-payer system delivering good-quality universal coverage as well as significantly reduced overall health-care spending? We can summarize their perspectives briefly.
Good-quality universal coverage
The CBO is clear, first of all, that a single-payer system would achieve universal coverage, in dramatic contrast with our present system. The report states, "People who are currently uninsured would receive coverage and some people who are currently insured could receive additional benefits under the single-payer system, depending on its design." In other words, a single-payer system would provide coverage for the 114 million U.S. residents who are presently either uninsured or underinsured. Healthcare outcomes for these 114 million people--35 percent of the U.S. population--will therefore almost certainly improve under a single-payer system.
The CBO does not take an explicit position as to whether a single-payer system will also deliver benefits for the 65 percent of the population which presently has full health-insurance coverage. On the one hand, the report does note both the prospects for both improved outcomes as well as reduced costs as regards this population cohort, observing that:
Unlike private insurers, which can experience substantial enrollee turnover over time, a single-payer system without that turnover would have a greater incentive to invest in measures to improve people's health and in preventive measures that have been shown to reduce costs.
It is also the case that both the Jayapal and Sanders bills offer more extensive coverage than is currently provided under a typical employer-sponsored policy, including significant support for long-term care. Expanding coverage in such ways should further improve overall health outcomes for those already insured. But the CBO also recognizes that the expansion of coverage to the uninsured and underinsured will entail increased overall demands on the country's supply of health care resources. It is therefore possible, as the report notes, that this could produce shortages in terms of availability of providers, which, in turn, could mean reductions in quality of care. This is a legitimate issue which the CBO has properly highlighted.
More specifically, the single-payer system will need to be capable of establishing measures through which the provision of provider services can increase to match the increased demand resulting from universal coverage. I examined this question in depth in a 200-page peer-reviewed study with co-authors released last November, "Economic Analysis of Medicare for All." In our study, we conclude that a single-payer system will produce major reductions in the administrative burdens throughout the whole health-care system. The CBO report also recognizes this prospect for major reductions in administrative burdens under single-payer. These dramatic cuts in administration will then mean significantly less paperwork for doctors and nurses, freeing them to spend more time treating patients. On balance, our study concluded that this effective increase in the providers' available time to treat patients should roughly match the increased demand for their services resulting from universal coverage.
Reducing Health-Care Costs
Much of the CBO report is focused around specific issues in designing the payment system. These include: provider payment methods; global budgets; capitated payments; payment rates for providers; and the setting of prescription drug prices. These are all critical concerns, and the CBO report is now a valuable resource in summarizing them. But the report does not take a position as to whether a U.S. single-payer system will be able to successfully control costs. Rather, the study concludes that:
The cost of a single-payer system would depend on various design choices such as the services covered, cost-sharing requirements, and provider payment rates.
In addition to those design choices, policymakers could consider using two other techniques to contain the growth of government spending on the single-payer plan and total health care spending: global budgets and utilization management. (p.26)
The CBO assessment here is indisputable. It is therefore incumbent on the designers of a single-payer system to consider the range of design choices with great care, to achieve the potential cost savings that are available through a well-designed system. It is evident from comparing the U.S. health care system with those of other high-income economies that there is massive potential for cost savings in the U.S. system, with, as noted above, the comparison countries spending between 9 - 11 percent of GDP on health care while the U.S. spends 17 percent. Within the present U.S. economy, every percentage point of GDP amounts to roughly $200 billion. Thus, even reducing our current health care spending by 2 percentage points relative to GDP would yield an astronomical $400 billion in savings, even while our healthcare system budget, as a share of GDP, would remain far above those of other advanced economics.
The CBO study is therefore to be commended for describing a range of measures through which a U.S. single-payer system can successfully implement significant cost savings while still delivering good-quality care for all residents. As such, the CBO study makes a positive contribution toward understanding the possibilities for creating a fair and workable health care system in the United States.
The Congressional Budget Office issued a report on May 1, 2019 titled "Key Design Components and Considerations for Establishing a Single-Payer Health Care System." This report reviews a range of considerations as regards the design and implementation of a single- payer system as applied to the United States. The Medicare for All bills currently before both the U.S. House of Representatives and Senate, as introduced by Representative Pramila Jayapal and Senator Bernie Sanders respectively, both advocate the adoption of a single-payer system for the U.S.
The CBO report (pdf) properly examines both the positive potential as well as matters of concern in establishing a single-payer system in the U.S. As the report states, "A single-payer system would present both opportunities and risks for the health care system."
Overall, the CBO report, as with all such analyses, needs to address two fundamental issues with respect to the establishment of a single-payer system for the U.S. These are: 1) Is a single-payer system capable of providing good-quality care to all U.S. residents; and 2) Is a single-payer system capable of significantly reducing overall U.S. health care costs while still delivering universal good-quality care? The report does not provide explicit answers, yes or no, to these questions. But it does present a framework for understanding how the U.S. could, in fact, establish a successful single-payer system.
"A single-payer system would provide coverage for the 114 million U.S. residents who are presently either uninsured or underinsured. Healthcare outcomes for these 114 million people--35 percent of the U.S. population--will therefore almost certainly improve under a single-payer system."
It is crucial to provide some context for recognizing the potential of a U.S. single- payer system as presented within the CBO report. It is especially illuminating to consider some basic indicators on the operations of the current U.S. health care system in comparison with those of other high-income economies. Thus, as of 2017, the U.S. spent $3.3 trillion on health care. This equaled 17 percent of US GDP, with average spending at about $10,000 per person. By contrast, Germany, France, Japan, Canada, the UK, Australia, Spain and Italy spent between 9 - 11 percent of GDP on health care, averaging between $3,400 - $5,700 per person. Yet, by most measures--including those based on the "amenable mortality rate," which tracks medically preventable deaths--average health outcomes in all of these countries are superior to those in the UnitedStates.
The most basic cause of this poor U.S. performance is inadequate access to good- quality care. Roughly 9 percent of the U.S. population, 28 million people, are uninsured. Another 26 percent, 86 million people, are underinsured--i.e. they have insurance but are unable to access medical care because their deductibles or co-pays are prohibitively high. A large share of the remaining 65 percent of the population who are adequately insured still face high costs as well as anxiety over whether they could manage financially when they face any serious health issue.
Within this context, how, then, does the CBO assess the prospects for a U.S. single-payer system delivering good-quality universal coverage as well as significantly reduced overall health-care spending? We can summarize their perspectives briefly.
Good-quality universal coverage
The CBO is clear, first of all, that a single-payer system would achieve universal coverage, in dramatic contrast with our present system. The report states, "People who are currently uninsured would receive coverage and some people who are currently insured could receive additional benefits under the single-payer system, depending on its design." In other words, a single-payer system would provide coverage for the 114 million U.S. residents who are presently either uninsured or underinsured. Healthcare outcomes for these 114 million people--35 percent of the U.S. population--will therefore almost certainly improve under a single-payer system.
The CBO does not take an explicit position as to whether a single-payer system will also deliver benefits for the 65 percent of the population which presently has full health-insurance coverage. On the one hand, the report does note both the prospects for both improved outcomes as well as reduced costs as regards this population cohort, observing that:
Unlike private insurers, which can experience substantial enrollee turnover over time, a single-payer system without that turnover would have a greater incentive to invest in measures to improve people's health and in preventive measures that have been shown to reduce costs.
It is also the case that both the Jayapal and Sanders bills offer more extensive coverage than is currently provided under a typical employer-sponsored policy, including significant support for long-term care. Expanding coverage in such ways should further improve overall health outcomes for those already insured. But the CBO also recognizes that the expansion of coverage to the uninsured and underinsured will entail increased overall demands on the country's supply of health care resources. It is therefore possible, as the report notes, that this could produce shortages in terms of availability of providers, which, in turn, could mean reductions in quality of care. This is a legitimate issue which the CBO has properly highlighted.
More specifically, the single-payer system will need to be capable of establishing measures through which the provision of provider services can increase to match the increased demand resulting from universal coverage. I examined this question in depth in a 200-page peer-reviewed study with co-authors released last November, "Economic Analysis of Medicare for All." In our study, we conclude that a single-payer system will produce major reductions in the administrative burdens throughout the whole health-care system. The CBO report also recognizes this prospect for major reductions in administrative burdens under single-payer. These dramatic cuts in administration will then mean significantly less paperwork for doctors and nurses, freeing them to spend more time treating patients. On balance, our study concluded that this effective increase in the providers' available time to treat patients should roughly match the increased demand for their services resulting from universal coverage.
Reducing Health-Care Costs
Much of the CBO report is focused around specific issues in designing the payment system. These include: provider payment methods; global budgets; capitated payments; payment rates for providers; and the setting of prescription drug prices. These are all critical concerns, and the CBO report is now a valuable resource in summarizing them. But the report does not take a position as to whether a U.S. single-payer system will be able to successfully control costs. Rather, the study concludes that:
The cost of a single-payer system would depend on various design choices such as the services covered, cost-sharing requirements, and provider payment rates.
In addition to those design choices, policymakers could consider using two other techniques to contain the growth of government spending on the single-payer plan and total health care spending: global budgets and utilization management. (p.26)
The CBO assessment here is indisputable. It is therefore incumbent on the designers of a single-payer system to consider the range of design choices with great care, to achieve the potential cost savings that are available through a well-designed system. It is evident from comparing the U.S. health care system with those of other high-income economies that there is massive potential for cost savings in the U.S. system, with, as noted above, the comparison countries spending between 9 - 11 percent of GDP on health care while the U.S. spends 17 percent. Within the present U.S. economy, every percentage point of GDP amounts to roughly $200 billion. Thus, even reducing our current health care spending by 2 percentage points relative to GDP would yield an astronomical $400 billion in savings, even while our healthcare system budget, as a share of GDP, would remain far above those of other advanced economics.
The CBO study is therefore to be commended for describing a range of measures through which a U.S. single-payer system can successfully implement significant cost savings while still delivering good-quality care for all residents. As such, the CBO study makes a positive contribution toward understanding the possibilities for creating a fair and workable health care system in the United States.